
Markets of Death, Part Two: Blood Permits – how cheating officials undermine wildlife regulations
March 14, 2016
Struggling Eastern Cape school told to take in more pupils
March 15, 2016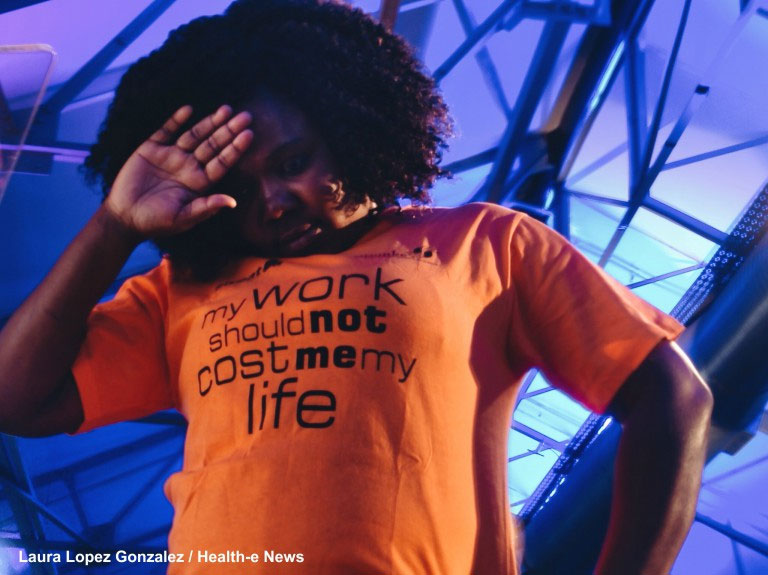
More than three million South Africans are on antiretrovirals (ARVs) today but even the world’s largest HIV treatment programme has been unable to reach those who live in society’s forgotten corners where HIV thrives among darkness and death.
Now, a rare mix of political will and science may be able to drive the virus out into the light, and possibly changing the lives of thousands
Promise Ngobeni lost her parents to AIDS-related illnesses as a child. The virus that robbed Ngobeni of her parents has stalked her since she began working as a sex worker in a Nelspruit club as a teen.
“I joined a group of teens and started going to night clubs looking for easy money,” she said. “If clients refuse to put on a condom on – even though some are HIV positive and some have sexually transmitted infections (STIs) – you cannot force them (to) because that client can report you to the boss.”
“You may lose your job or your boss can beat you to death,” she added. “Some of us joined the prostitution industry HIV negative but now we are HIV positive.
On Friday, South Africa announced that it would become one of the world’s first countries to begin providing the combination ARV Truvada to at least 3,000 HIV-negative sex workers to help prevent them from contracting HIV. Combining the ARVs emtricitabine and tenofovir, daily Truvada has been shown to reduce a person’s risk of contracting HIV by more than 90 percent when used as pre-exposure prophylaxis (PrEP).
Friday’s announcement comes as a recent study conducted among 2,200 female sex workers in Johannesburg, Cape Town and Durban that found about 72 percent of women surveyed were living with HIV. Although more than 90 percent of sex workers surveyed had tested for HIV, less than a third of those living with HIV were on ARVs– far less than the national average, according to South Africa National AIDS Council (SANAC) CEO Dr Fareed Abdullah.
To combat low uptake of treatment, sex workers will now be able to start HIV treatment as soon as they are diagnosed with HIV – a model of care known as “test and treat”. Currently, most people living with HIV must wait until their CD4 counts – a measure of the immune system’s strength – fall to 500 before they starting treatment.
Early HIV treatment is not only better for people living with HIV, it may also help HIV-positive people bring the level of HIV in their blood down sooner. When levels fall so low that they are termed “undectable” by HIV viral load testing, people are much less likely to transmit HIV to their partners.
The World Health Organisation (WHO) endorsed both PrEP as well as test and treat in September.
The changes in HIV treatment policies for sex workers are part of South Africa’s first national plan to address the HIV epidemic among sex workers. Announced by Deputy President and SANAC Chair Cyril Ramaphosa amid choruses of toyi-toying sex workers armed with dildos and grape-scented condoms, the plan is a first in Africa. It also heralds the most significant move to address HIV in South Africa since the introduction of ARV treatment in 2004.
“We cannot reclaim the morality of society by excluding the most vulnerable, whatever views we might have about sex workers, whatever beliefs we have about sex workers, whatever statutes are on our law books about the legality of sex work,” Ramaphosa said. “We cannot deny the human and unalienable rights of people who engage in sex work.”
“Sex work is essentially work,” he said.
About one in five sex workers surveyed in the University of California study had been sexually assaulted in the last year.
Tracking a virus amongst the shadows
If you succeed in national (HIV) programmes and scale ups, you begin to push the epidemic into corners. In those corners, there is not a lot of light and people are living in the shadows still with darkness and death”
South Africa’s decision to provide PrEP to sex workers is part of a growing international trend to address high HIV prevalence rates in high-risk and often marginalised populations.International donors like the Global Fund to Fight AIDS, Tuberculosis and Malaria is increasingly pushing countries to address groups like sex workers, injecting drug users and young women in national programmes not only because it promotes human rights but because it’s just good science.
“What the epidemiology is telling us is that… if you succeed in national (HIV) programmes and scale ups, you begin to push the epidemic into corners,” said Global Fund Executive Director Mark Dybul in a 2013 interview. “In those corners, there is not a lot of light and people are living in the shadows still with darkness and death. Those are usually the people most marginalized in society, and who don’t have access to care.”
“Just building clinics and making healthcare available gets to a lot of people, but it doesn’t get to the people who are beyond the reach of clinics – that really means getting to the most vulnerable,” Dybul added.
There is perhaps no better branch of science than epidemiology to show us how closely connected we really are to the people we often judge and other.
As many as 20 percent of new HIV infections in South Africa may be linked to sex work, according to Deputy Health Minister Joe Phaahla.
Sex workers may just be the start
We may be creating a social construct that PrEP is for these ‘bad people’ who are disorganised and are thought to be having a lot of sex. What we should be doing is targeting anyone who is at high risk of HIV”
In many countries, epidemiology is pushing governments to work with criminalised populations like sex workers and men who have sex with men to step HIV epidemics. For many politicians, it’s an uncomfortable partnership of necessity that in some African countries means that health departments are quietly undertaking small programmes to reach out to these groups without much public pomp and circumstance.South Africa’s high-level and very public commitment to addressing HIV among sex workers is a rarity.
“It’s rare for a country to have such high-level leadership dealing with HIV among sex workers,” Abdullah said. “It’s a sign that government is taking this very seriously and working with non-governmental organisations and the community to make sure that the right thing is done and done properly.
And PrEP for sex workers may be just the beginning.
Prior to the announcement, both the Wits Reproductive Health and HIV Institute (WRHI) and the Anova Health Institute had started small demonstration projects aimed at learning how best PrEP might be rolled out. While WRHI focused on Hillbrow sex workers, Anova Health nurses have been providing PrEP to about 100 men who have sex with men (MSM) from its Woodstock clinic in Cape Town.
Previous 2009 studies conducted in Johannesburg and Durban, as many as about 38 percent of MSM surveyed were living with HIV – a figure almost double the national adult HIV prevalence rate.
With a growing body of data on the country’s MSM, as well as new lessons being learned in Woodstock, MSMs may be the next group to receive PrEP if South Africa continues rolling out the once-a-day pill for prevention.
PrEP’s real test may be young women
The real test for PrEP in South Africa may eventually be whether the country can figure out how to provide it to one of the country’s highest risk groups: Young women.Young women between the ages of 15 and 24 years old are more than four times more likely than men in their age group to be living with HIV, according to the latest Human Science Research Council household HIV survey. Women in this age bracket also account for about a quarter of all new infections in South Africa.
Dr Kevin Rebe is a specialist medical consultant for the Anova Health Institute in Cape Town. Rebe worries that how we talk about PrEP now, may affect how young women see the prevention option tomorrow.
With initial rollouts focused on highly stigmatised populations like sex workers and perhaps later MSM, Rebe cautions that there may be a risk that PrEP itself becomes stigmatised.
“We may be creating a social construct that PrEP is for these ‘bad people’ who are disorganised and are thought to be having a lot of sex,” he said. “If this happens, we may get a backlash against PrEP.
“How do we prevent shaming people who are actually doing something responsible for their health?” he asked. “That’s a real danger.
“What we should be doing is targeting anyone who is at high risk of HIV,” said Rebe, adding that following Truvada’s 2015 Medicines Control Council approval for use as prevention there is nothing stopping private sector patients from asking doctors if PrEP is right for them.
Medical aid Fedhealth has already said it will cover at least six months of PrEP for medical scheme members who are at a high risk of HIV as well those who are in relationships with HIV-positive partners.
For the SA Medical Research Council’s Head of AIDS Research Dr Gita Ramjee, the first step in talking about young women and PrEP is understanding young women.
“In all the bio-medial interventions we’ve tried and tested with young women, the main reason for them not working was because of low adherence in this group,” said Ramjee, who added small demonstration projects conducted among young women – like those already being conducted with sex workers and MSM – would be needed to understand everything from women’s desires and emotions to how they perceive their HIV risk.
“Emotion and desire are very important drivers of decision-making process for this group,” Ramjee toldHealth-e News. “Once we understand the social, cultural and economic context and the emotions underneath what these young women are feeling and believing… what their need for HIV prevention is then we’d be ready to send a message out to young people.”
In the meantime, PrEP may be a conversation that’s worth having for everyone. – Health-e News.
Additional reporting by Cynthia Maseko. An edited version of this story also appeared on the Daily Maverick.




{kind=link}
{kind=link}
{kind=link}
{kind=link}